Is It Really Diabetes or a Liver Problem? How to Tell When Symptoms Overlap

You're tired all the time. You get thirsty more than usual. Your weight shifts, even though you haven't changed much. Then routine labs come back "off," and suddenly you're staring at two scary possibilities: diabetes, a liver issue, or both.
Here's the uncomfortable truth: diabetes and liver trouble can feel the same at first. The liver helps manage blood sugar every day, so when it's stressed, glucose numbers can drift. At the same time, high blood sugar can strain the liver. That's why guessing based on symptoms alone often leads people in the wrong direction.
This guide lays out a clear plan: what overlap symptoms mean, which liver warning signs shouldn't be ignored, what tests help doctors sort it out, and what you can do next. If you want a steady starting point for basics, the Waldrugmart Health Guide is a practical place to learn the language before your next appointment.
 Fatigue and thirst can show up with high blood sugar, liver stress, or both (created with AI).
Fatigue and thirst can show up with high blood sugar, liver stress, or both (created with AI).
https://www.youtube.com/watch?v=upOU_EEXsBA
Why diabetes and liver problems can look so similar
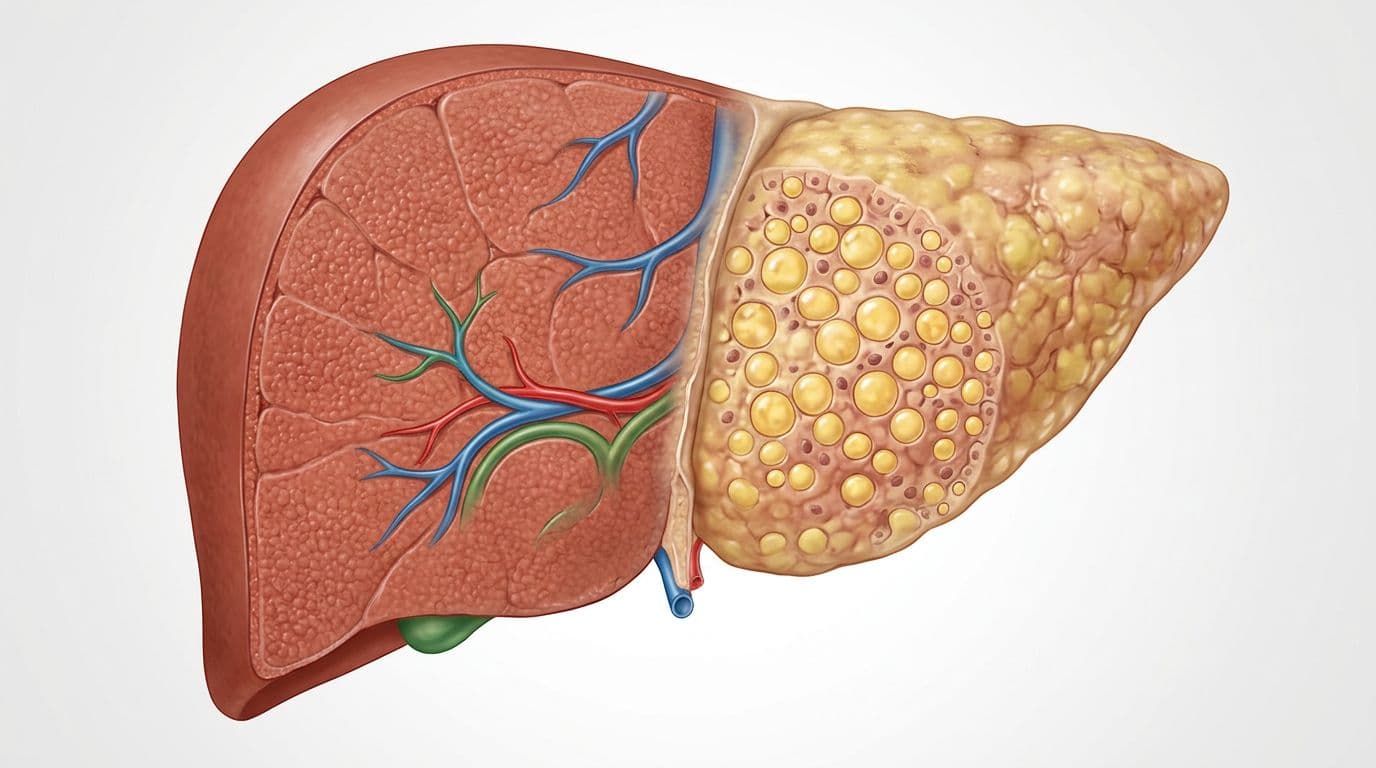 Fat buildup in the liver can change how your body handles sugar (created with AI).
Fat buildup in the liver can change how your body handles sugar (created with AI).
Think of the liver as your body's "pantry manager." It stores sugar as glycogen, then releases it between meals. It also helps clear insulin and keeps many chemical reactions steady. Because of that, a struggling liver can throw off blood sugar even if you don't have classic diabetes yet.
Now flip it around. When blood sugar stays high, the liver often gets pulled into the problem. It may start making and releasing extra glucose, especially overnight. That can push fasting numbers up. You wake up feeling drained, and it's easy to blame stress, age, or a bad week of sleep.
Confusion happens because both conditions share a "quiet phase." Early type 2 diabetes can be subtle. Early fatty liver disease can be silent. Meanwhile, the symptoms people notice first are often broad: low energy, appetite changes, or unexplained weight shifts.
This overlap is so common that major diabetes groups now push for liver screening in people with type 2 diabetes and prediabetes. The reasoning is simple: you can't manage one problem well while missing the other. For the clinical big picture, see the American Diabetes Association consensus on steatotic liver disease in people with diabetes.
The shared symptoms that can fool you
Fatigue is the classic trap. When glucose runs high, cells can't use fuel well, so you feel like you're running on low battery. When the liver is inflamed or stressed, fatigue can also hit hard, even after a full night's sleep.
Weight changes can confuse things, too. Some people lose weight with untreated diabetes because the body can't use glucose properly. On the other hand, long-term insulin resistance often links with weight gain, which also raises the chance of fatty liver.
Loss of appetite fits both stories. Blood sugar swings can blunt hunger or cause nausea. Liver stress can do the same, especially if bile flow or digestion feels "off." Many people describe a vague feeling of being worn out after meals, like they crash after lunch and can't focus.
Thirst and frequent urination point more strongly to high blood sugar, especially if they're new and persistent. Still, they can show up with other health stressors. Dehydration, infection, and some medications can mimic parts of the picture.
Self-diagnosing is risky because the overlap is real. The same symptom can come from different causes, and the fix depends on the cause.
How fatty liver ties into insulin resistance
Fatty liver disease (often called MASLD today, and previously NAFLD) means fat builds up in the liver even without heavy drinking. It's common, and it's not a character flaw. It's often the result of long-term metabolic pressure, like insulin resistance, higher triglycerides, or weight gain over time.
When fat accumulates in the liver, the liver often stops responding to insulin's "slow down" signal. As a result, it keeps releasing glucose into the blood, even when you don't need it. That can raise fasting glucose and A1C, sometimes before you feel anything dramatic.
As of March 2026, estimates suggest MASLD affects roughly 65 to 70% of adults with type 2 diabetes, and many also have the more severe inflammatory form (often called MASH). In other words, this is frequently not an either-or problem.
That's also why treatment often overlaps. Better glucose control can help liver outcomes, and better liver habits can improve insulin sensitivity. Some diabetes medications may even help reduce liver fat for some patients, although your clinician has to match the option to your full health profile. If you're already managing type 2 diabetes, Waldrugmart's guide on Rybelsus semaglutide for type 2 diabetes can help you understand what to discuss at follow-ups.
For a deeper explanation of the insulin resistance link across disease stages, review the research summary on insulin resistance in fatty liver disease.
Clues that point more toward a liver issue (not just diabetes)
 Yellowing of the eyes or skin is a classic liver warning sign (created with AI).
Yellowing of the eyes or skin is a classic liver warning sign (created with AI).
Diabetes can cause serious problems, but it usually doesn't turn your eyes yellow. Liver disease has a few signals that stand out because they relate to bile flow and liver function, not just sugar control.
At the same time, early liver disease can show no symptoms at all. That's why lab work matters, even when you feel "fine." It's also why a normal day-to-day routine can mask a growing problem, until something finally tips.
If you notice yellowing of the eyes, vomiting blood, black tar-like stools, severe confusion, or a rapidly swollen belly, treat it as urgent and seek emergency care.
Signs your liver may be struggling
Some symptoms deserve extra respect because they point more directly to liver stress or advanced disease. This table helps you sort urgency at a glance.
| Symptom | What it can suggest | How fast to act |
|---|---|---|
| Yellow skin or eyes (jaundice) | Bilirubin buildup, bile flow issues | Same day evaluation |
| Right upper belly pain | Liver or gallbladder irritation | Prompt evaluation, urgent if severe |
| Belly swelling | Fluid buildup (ascites) | Urgent evaluation |
| Confusion or extreme sleepiness | Toxin buildup affecting the brain | Emergency care |
| Vomiting blood or bloody, black stools | GI bleeding | Emergency care |
Other clues can be quieter: easy bruising, itchy skin without a clear rash, dark urine, or very pale stools. None of these confirm a diagnosis alone. Still, they're strong reasons to get checked quickly.
One more "gotcha" matters: liver enzymes can be normal even with meaningful liver scarring. That's why clinicians may use risk scores and imaging, not only ALT and AST.
Medication, alcohol, and other causes that can stress the liver
Many things can strain the liver, and it's rarely one simple cause. Alcohol can play a role for some people, even at moderate levels if the liver is already vulnerable. Viral hepatitis risk also matters, especially if you've had past exposures through blood, unsterile needles, or certain medical settings. Long-term metabolic issues, including high blood sugar and high triglycerides, can add pressure year after year.
Medications and supplements can also contribute. The liver processes many compounds, so stacking products can raise risk, especially if you mix prescriptions, over-the-counter pain relievers, herbals, and "wellness blends." That risk rises further if you're on complex regimens, including cancer medications, where drug interactions matter more.
Bring this short checklist to your visit:
- All prescriptions (including dose and how often you take them)
- Over-the-counter meds (especially pain relievers, sleep aids, cold meds)
- Herbals and vitamins (even "simple" ones)
- Any Liver Detox product or cleanse tea, because "natural" doesn't always mean safe
A trusted Online Pharmacy can help you double-check interactions and refill timing, especially when multiple specialists prescribe medications. Similarly, a reputable Online chemist with pharmacist review can be a practical backstop, so you're not guessing about combinations.
If your clinician suspects a bile flow disorder (a different issue than fatty liver), you may hear about medicines that support bile movement. Waldrugmart's explainer on UDCA dosing and side effects guide can help you understand that conversation without getting lost in jargon.
The tests that help doctors tell the difference, and why you may need both
 Blood tests can confirm diabetes, show liver stress, and guide next steps (created with AI).
Blood tests can confirm diabetes, show liver stress, and guide next steps (created with AI).
If symptoms were enough, no one would need lab work. In real life, clinicians rely on numbers because fatigue, appetite loss, and weight changes can come from dozens of causes.
A good evaluation often checks both "sides of the house":
- Blood sugar status (to confirm diabetes, prediabetes, or normal control)
- Liver injury and function (to spot inflammation, bile flow issues, or reduced liver output)
- Fibrosis risk (to estimate scarring and decide on imaging)
This matters because people can have type 2 diabetes and fatty liver at the same time. Also, a person can have liver disease without diabetes and still show mild glucose changes during illness.
For a thorough medical review of screening and management in type 2 diabetes, this open-access paper on fatty liver disease in patients with type 2 diabetes explains why clinicians often screen earlier than patients expect.
Blood sugar tests that confirm diabetes (or rule it out)
Three tests do most of the heavy lifting:
Fasting plasma glucose checks your blood sugar after not eating overnight. A fasting glucose of 126 mg/dL or higher on testing suggests diabetes (your clinician may repeat it to confirm). Lower levels can still mean prediabetes, depending on the exact number.
A1C reflects your average blood sugar over about three months. It's helpful because it doesn't swing as much day to day. However, some blood disorders and certain medical situations can affect A1C accuracy, so your clinician may choose a different test if needed.
Oral glucose tolerance test (OGTT) measures how your body handles sugar over a few hours after a sugary drink. It's especially useful when fasting glucose and A1C don't match the story.
Symptoms alone don't confirm diabetes. Also, stress, infections, steroid medicines, and other short-term factors can temporarily raise glucose. If your numbers look borderline, repeat testing can prevent a wrong label.
Liver labs and scoring tools that show liver stress or scarring risk
Liver blood tests often come in a "panel," and each marker tells a slightly different story:
- ALT and AST can rise when liver cells are irritated or inflamed.
- ALP and GGT can rise when bile flow slows or bile ducts are stressed.
- Bilirubin can rise when the liver can't clear it well, which links with jaundice.
- Albumin reflects protein-making capacity, and low levels can signal reduced liver function (especially in more advanced disease).
Because enzyme levels don't always match scarring, clinicians often use a simple risk score called FIB-4. It uses age and basic labs (including AST, ALT, and platelets) to estimate the chance of significant fibrosis. A higher-risk score doesn't prove cirrhosis, but it often triggers follow-up testing, such as an ultrasound, elastography (FibroScan), or other imaging.
A newer study summary also supports using non-invasive markers earlier in people with obesity and metabolic syndrome. If you want the research angle, see this report on non-invasive fibrosis markers in NAFLD.
Here are three practical questions to bring to your clinician:
- Do I need liver screening if I have type 2 diabetes or prediabetes?
- Should we calculate FIB-4 from my labs?
- Based on my risk, should I get an ultrasound or other imaging?
The goal isn't to collect tests. The goal is follow-up, so one abnormal result becomes a plan, not a mystery.
Conclusion: Don't guess, check both
When fatigue, appetite changes, and weight shifts hit together, it's tempting to pick one explanation. Still, diabetes and liver problems overlap so much that guessing can waste months. The calm approach is also the fastest.
Use this simple 4-step plan: track symptoms for two weeks, request both glucose and liver labs, review every medication and supplement (including any Liver Detox product), then follow a realistic routine while you wait, steady sleep, balanced meals, gentle activity, and less alcohol. If you already take several prescriptions, especially for chronic illness, a pharmacist review can prevent avoidable problems.
For education you can trust between visits, use the Waldrugmart Health Guide as your plain-language reference point. When you need refills or interaction checks, choose a trusted Online Pharmacy that verifies prescriptions and offers pharmacist support. Your next step doesn't need to be perfect, it just needs to be informed.